

Chest X-ray and Computed tomography (CT or CAT scan)
Chest X- rays are a form of high-energy radiation that penetrates through the body, capturing images on film.
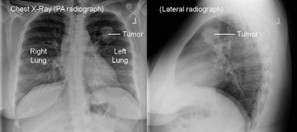
A chest X-ray specifically captures images of the bones in the chest and spine, as well as the internal organs within the chest cavity, such as the lungs, airways, heart, and blood vessels.
Typically, when symptoms are non-specific, a doctor frequently relies on a chest X-ray as the initial examination to identify any growths. Nonetheless, chest X-rays frequently fail to detect small lung cancers during the early phases of the disease. If there is suspicion of lung cancer, it is advisable to inquire about a CT scan from your doctor instead of, or alongside, a chest X-ray.
Computed tomography (CT or CAT scan)
Computed tomography (CT) uses a computer connected to an X-ray machine to generate detailed images of the body’s internal structures. Unlike traditional X-rays, which capture a single image, a CT scanner captures multiple images by rotating around the patient, acquiring views from various angles. This process enables the creation of three-dimensional (3D) images of organs and tissues.

A CT scan offers precise information regarding the size, shape, and location of growths or nodules within the lungs. Additionally, it aids in identifying enlarged lymph nodes or masses in other organs, raising concerns of lung cancer metastasis. It is important to understand that while a CT scan effectively reveals the presence of abnormalities, it does not provide a definitive diagnosis; further tests are necessary for accurate diagnosis.
In some cases, patients may drink a contrast solution or receive intravenous dye before a CT scan in order to define accuratelyorgans and blood vessels. During the procedure, it is imperative for the patient to remain still, and occasionally, they may be asked to hold their breath briefly. CT scans typically require only a few minutes to complete.
Presently, low-dose CT scans (LDCT) are commonly employed for lung cancer screening and monitor changes in lung nodules. LDCT involves a radiation dose approximately five times lower than that of a standard CT scan.

Magnetic resonance imaging (MRI)
MRI scans offer images of internal body regions, utilizing radio waves and powerful magnets. Radio wave energy is absorbed and subsequently emitted in a pattern that a computer deciphers into visual representations. Typically, an intravenous injection of contrast dye precedes the MRI to enhance image clarity.
The scanner usually consists of a narrow tube where the patient reclines. While there are “open” MRI machines designed for individuals with claustophobia, the resulting images may not always be sharp. Compared to a CT scan, an MRI scan typically requires more time, occasionally lasting up to 50 minutes. Patients are provided with earplugs or earmuffs to isolate the loud banging noises produced during the scans.
In lung cancer, magnetic resonance imaging (MRI) is used to determine whether the cancer has spread to the brain or spinal cord.
Positron emission tomography (PET-CT scan)
The PET-CT scan determines whether or not an abnormal finding on a chest X-ray or CT scan has increased metabolic activity (i.e. whether it is an active lesion and possibly cancer, infection or inflammation, or whether it is an inactive lesion possibly due to an earlier disease or simply an old scar).
The patient is given an intravenous radioactive sugar similar to glucose. Because cancer cells have a rapid metabolism, they absorb more radioactive glucose than most healthy cells. About an hour after the injection, a special camera captures the radiation of the radioactive glucose absorbed by the patient’s body and creates an image of the abnormal areas throughout the body.
As the PET-CT scan is a full-body scan, it defines the stage of the disease, as it gives us information on whether there is spread of the cancer to lymph nodes, bones or other organs throughout the body. However, PET scans are not used to investigate the brain as brain cells absorb a large amount of sugar and therefore we can get false positive results.
The PET-CT scan (combined PET and CT scan) that is generally used today cannot always distinguish between a benign inflammation, infection or malignant disease. Therefore biopsies are required to accurately and safely determine the final diagnosis, when a finding of unknown cause appears.
Bone scan
A bone scan operates similarly to a PET scan, involving the injection of a small quantity of radioactive tracer into a vein. Over the course of a few hours, the tracer accumulates in areas of bone affected by injury, including those resulting from cancer. Subsequently, the patient reclines on a table for approximately 30 minutes while a camera captures the radioactivity and generates an image of the skeletal structure.
Given that PET scans can also detect cancer within the bones, they are typically preferred over bone scans in cases of lung cancer.